



This is part of a series of guest posts about the Covid-19 crisis by Dr. Felicia Keesing, an expert in disease ecology. Please note that the situation is continually evolving and information may become out-of-date.
Basic virus biology
Viruses aren’t cells, and they’re not living organisms. They’re parasitic particles that hijack the cells of living organisms and use these cells to make more copies of themselves. A virus particle basically consists of a fatty membrane with a bit of DNA or RNA inside. The fatty membrane has proteins embedded in it which help the virus invade the cells it will parasitize. For more on the specific components of SARS-CoV-2, the coronavirus that causes Covid-19, check out this amazing infographic.
A virus first has to get into a host so that it can hijack the host’s cells. Viruses generally get from one host to another through the host’s bodily fluids, so the virus particles in the bodily fluids of the infected host have to come into contact with the bodily fluids of a new host. Some viruses travel in blood, others in saliva or mucus, others in feces or urine. SARS- CoV-2 appears to travel to new hosts through saliva and mucus, and also through feces.
Once a virus invades a new host, it takes some time before it begins making copies of itself. That’s called the incubation period. After the incubation period, the virus begins making copies of itself and starts to spread within the host. At this point, it can also spread to new hosts. This is called the infectious period. The immune system of an infected host is typically fighting the virus, and if all goes well, the immune system will eventually destroy the virus particles. At that point, the host is recovered, and may be immune to reinfection, depending on the specific virus. In some cases, the immune system is never able to fight off the virus, as is the case for HIV. We know that the immune system can fight off SARS-CoV- 2, though, so there’s a bit of good news.
With this basic background, we can begin asking how SARS-CoV-2 is different from other viruses that cause disease in humans. As my points of comparison, I’ll primarily use two other coronaviruses – the viruses that cause SARS (Severe Acute Respiratory Syndrome) and MERS (Middle East Respiratory Syndrome) – and the influenza virus that causes the flu, with guest appearances by other notorious viruses like Ebola virus and HIV.
How long is the incubation period?
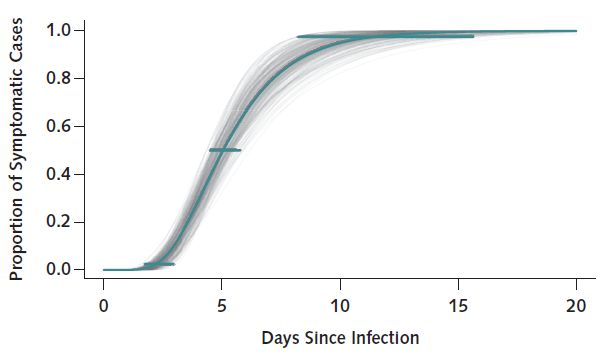
The average incubation period of SARS-CoV-2 is about 5 days, though it can be as long as 14 days, and perhaps a bit longer. This is longer than the 1-3 day incubation period for influenza, for example, but shorter than the 9-21 day incubation period for the virus that causes chicken pox, or the much, much longer incubation period for HIV (for a simple table). So this virus doesn’t have an unusual incubation period.
How infectious is it?
Epidemiologists measure the rate at which a virus spreads with a measure called Ro (which is pronounced R-nought). Ro is the number of new infections that arise from a single infected host. Ro for measles is 12-18, meaning that a single infected person typically infects 12-18 others. Ro for the 1918 influenza virus was 1.8, for Ebola it’s about 2, for the common cold virus it’s 2-3. For SARS- CoV-2, it’s 1.4-3.9. But back in 2002, the first SARS virus had a similar Ro, yet was much more easily contained. In sum, SARS-CoV-2 doesn’t stand out for its infectiousness.
(Note that we’re practicing social distancing in an effort to reduce the Ro of the virus. If we can get Ro below 1, there will be fewer and fewer infected hosts over time and the infection will die out.)


